
Task E. Physiology
| Task E. Physiology | |
| References | AC 107-2; FAA-H-8083-2, FAA-H-8083-25; FAA-G-8082-22 |
| Objective | To determine that the applicant is knowledgeable in the physiological factors affecting remote pilot performance. |
| Knowledge | The applicant demonstrates understanding of: |
| UA.V.E.K1 | Physiological considerations and their effects on safety such as dehydration and heatstroke. |
| UA.V.E.K2 | Drug and alcohol use. |
| UA.V.E.K3 | Prescription and over-the-counter medication. |
| UA.V.E.K4 | Hyperventilation. |
| UA.V.E.K5 | Stress and fatigue. |
| UA.V.E.K6 | Factors affecting vision. |
| UA.V.E.K7 | Fitness for flight. |
| UA.V.E.K8 | Physiological aspects of night operation. |
| UA.V.E.K9 | Night illusions. |
| Risk Management | [Reserved] |
| Skills | [Not Applicable] |
UA.V.E.K1 Physiological considerations and their effects on safety such as dehydration and heatstroke (AC 107-2A)
Dehydration
Dehydration is the term given to a critical loss of water from the body. Causes of dehydration are hot temperatures, wind, humidity, and diuretic drinks—coffee, tea, alcohol, and caffeinated soft drinks. Some common signs of dehydration are headache, fatigue, cramps, sleepiness, and dizziness.
The first noticeable effect of dehydration is fatigue, which in turn makes top physical and mental performance difficult, if not impossible. Flying a small UA for long periods in hot summer temperatures or at high altitudes increases the susceptibility to dehydration because these conditions tend to increase the rate of water loss from the body.
To help prevent dehydration, drink two to four quarts of water every 24 hours. Since each person is physiologically different, this is only a guide. Most people are aware of the eight-glasses-a-day guide: If each glass of water is eight ounces, this equates to 64 ounces, which is two quarts. If this fluid is not replaced, fatigue progresses to dizziness, weakness, nausea, tingling of hands and feet, abdominal cramps, and extreme thirst.
The key for pilots is to be continually aware of their condition. Most people become thirsty with a 1.5 quart deficit or a loss of 2 percent of total body weight. This level of dehydration triggers the “thirst mechanism.” The problem is that the thirst mechanism arrives too late and is turned off too easily. A small amount of fluid in the mouth turns this mechanism off and the replacement of needed body fluid is delayed.
Other steps to prevent dehydration include:
• Carrying a container in order to measure daily water intake.
• Staying ahead—not relying on the thirst sensation as an alarm. If plain water is not preferred, add some sport drink flavoring to make it more acceptable.
• Limiting daily intake of caffeine and alcohol (both are diuretics and stimulate increased production of urine).
Heatstroke
Heatstroke is a condition caused by any inability of the body to control its temperature. Onset of this condition may be recognized by the symptoms of dehydration, but also has been known to be recognized only upon complete collapse. To prevent these symptoms, it is recommended that an ample supply of water be carried and used at frequent intervals, whether thirsty or not. The body normally absorbs water at a rate of 1.2 to 1.5 quarts per hour. Individuals should drink one quart per hour for severe heat stress conditions or one pint per hour for moderate stress conditions. For more information on water consumption, refer to the “Dehydration” section of this chapter.
UA.V.E.K2 Drug and alcohol use (FAA-H-8083-25C Ch. 17)
Drugs
The Federal Aviation Regulations include no specific references to medication usage. Two regulations, though, are important to keep in mind. Title 14 of the CFR part 61, section 61.53 prohibits acting as pilot-in-command or in any other capacity as a required pilot flight crewmember, while that person:
1. Knows or has reason to know of any medical condition that would make the person unable to meet the requirement for the medical certificate necessary for the pilot operation, or
2. Is taking medication or receiving other treatment for a medical condition that results in the person being unable to meet the requirements for the medical certificate necessary for the pilot operation. Further, 14 CFR part 91, section 91.17 prohibits the use of any drug that affects the person’s faculties in any way contrary to safety.
Further, 14 CFR part 91, section 91.17 prohibits the use of any drug that affects the person’s faculties in any way contrary to safety.
(a) No person may act or attempt to act as a crewmember of a civil aircraft—
(1) Within 8 hours after the consumption of any alcoholic beverage;
(2) While under the influence of alcohol;
(3) While using any drug that affects the person’s faculties in any way contrary to safety; or
(4) While having an alcohol concentration of 0.04 or greater in a blood or breath specimen. Alcohol concentration means grams of alcohol per deciliter of blood or grams of alcohol per 210 liters of breath.
(b) Except in an emergency, no pilot of a civil aircraft may allow a person who appears to be intoxicated or who demonstrates by manner or physical indications that the individual is under the influence of drugs (except a medical patient under proper care) to be carried in that aircraft.
(c) A crewmember shall do the following:
(1) On request of a law enforcement officer, submit to a test to indicate the alcohol concentration in the blood or breath, when—
(i) The law enforcement officer is authorized under State or local law to conduct the test or to have the test conducted; and
(ii) The law enforcement officer is requesting submission to the test to investigate a suspected violation of State or local law governing the same or substantially similar conduct prohibited by paragraph (a)(1), (a)(2), or (a)(4) of this section.
(2) Whenever the FAA has a reasonable basis to believe that a person may have violated paragraph (a)(1), (a)(2), or (a)(4) of this section, on request of the FAA, that person must furnish to the FAA the results, or authorize any clinic, hospital, or doctor, or other person to release to the FAA, the results of each test taken within 4 hours after acting or attempting to act as a crewmember that indicates an alcohol concentration in the blood or breath specimen.
(d) Whenever the Administrator has a reasonable basis to believe that a person may have violated paragraph (a)(3) of this section, that person shall, upon request by the Administrator, furnish the Administrator, or authorize any clinic, hospital, doctor, or other person to release to the Administrator, the results of each test taken within 4 hours after acting or attempting to act as a crewmember that indicates the presence of any drugs in the body.
(e) Any test information obtained by the Administrator under paragraph (c) or (d) of this section may be evaluated in determining a person’s qualifications for any airman certificate or possible violations of this chapter and may be used as evidence in any legal proceeding under section 602, 609, or 901 of the Federal Aviation Act of 1958.
Anesthetic drugs are commonly used for dental and surgical procedures. Most local anesthetics used for minor dental and outpatient procedures wear off within a relatively short period of time. The anesthetic itself may not limit flying as much as the actual procedure and subsequent pain.
There is evidence taking illicit drugs significantly elevates the risk of having an aviation accident. Even though the Drug Enforcement Administration (DEA) defines marijuana as a Schedule I drug on its controlled substances list, states have taken steps to allow the possession, sale, and use of marijuana within their border. The FAA has stated, “Marijuana is an illicit drug per federal law and its use by airmen is prohibited.”
Stimulants are drugs that excite the central nervous system and produce an increase in alertness and activity. Amphetamines, caffeine, and nicotine are all forms of stimulants. Common uses of these drugs include appetite suppression, fatigue reduction, and mood elevation. Some of these drugs may cause a stimulant reaction, even though Stimulants are drugs that excite the central nervous system and produce an increase in alertness and activity. Amphetamines, caffeine, and nicotine are all forms of stimulants. Common uses of these drugs include appetite suppression, fatigue reduction, and mood elevation. Some of these drugs may cause a stimulant reaction, even though this reaction is not their primary function. In some cases, stimulants can produce anxiety and mood swings, both of which are dangerous when flying.
Depressants are drugs that reduce the body’s functioning in many areas. These drugs lower blood pressure, reduce mental processing, and slow motor and reaction responses. There are several types of drugs that can cause a depressing effect on the body, including tranquilizers, motion sickness medication, some types of stomach medication, decongestants, and antihistamines. The most common depressant is alcohol.
Some drugs that are classified as neither stimulants nor depressants have adverse effects on flying. For example, some antibiotics can produce dangerous side effects, such as balance disorders, hearing loss, nausea, and vomiting. While many antibiotics are safe for use while flying, the infection requiring the antibiotic may prohibit flying. In addition, unless specifically prescribed by a physician, do not take more than one drug at a time, and never mix drugs with alcohol because the effects are often unpredictable.
The dangers of illegal drugs also are well documented. Certain illegal drugs can have hallucinatory effects that occur days or weeks after the drug is taken. Obviously, these drugs have no place in the aviation community.
14 CFR prohibits pilots from performing crewmember duties while using any medication that affects the body in any way contrary to safety. The safest rule is not to fly as a crewmember while taking any medication, unless approved to do so by the FAA. If there is any doubt regarding the effects of any medication, consult an AME before flying.
Prior to each and every flight, all pilots must do a proper physical self-assessment to ensure safety. A great mnemonic, covered in Chapter 2 on Aeronautical Decision-Making, is IMSAFE, which stands for Illness, Medication, Stress, Alcohol, Fatigue, and Emotion.
For the medication component of IMSAFE, pilots need to ask themselves, “Am I taking any medicines that might affect my judgment or make me drowsy? For any new medication, OTC or prescribed, you should wait at least 48 hours after the first dose before flying to determine you do not have any adverse side effects that would make it unsafe to operate an aircraft. In addition to medication questions, pilots should also consider the following
• Do not take any unnecessary or elective medications;
• Make sure you eat regular balanced meals;
• Bring a snack for both you and your passengers for the flight;
• Maintain good hydration – bring plenty of water;
• Ensure adequate sleep the night prior to the flight; and
• Stay physically fit.
Additionally, you should wait at least five maximal dosing intervals, the time between recommended or prescribed dosing, (e.g., a dosing interval of 5 to 6 hours would require you to wait 30 hours) before flying after taking any medication that has potentially adverse side effects (e.g., sedating or dizziness). Observing the recommended dosing interval doesn’t eliminate the risk for adverse side effects because everyone metabolizes medications differently. However, five times the dosing interval is a reasonable rule of thumb.
Alcohol
Alcohol impairs the efficiency of the human body. [Figure 17-8] Studies have shown that consuming alcohol is closely linked to performance deterioration. Pilots must make hundreds of decisions, some of them time-critical, during the course of a flight. The safe outcome of any flight depends on the ability to make the correct decisions and take he appropriate actions during routine occurrences, as well as abnormal situations. The influence of alcohol drastically reduces the chances of completing a flight without incident. Even in small amounts, alcohol can impair judgment, decrease sense of responsibility, affect coordination, constrict visual field, diminish memory, reduce reasoning ability, and lower attention span. As little as one ounce of alcohol can decrease the speed and strength of muscular reflexes, lessen the efficiency of eye movements while reading, and increase the frequency at which errors are committed. Impairments in vision and hearing can occur from consuming as little as one drink.
The alcohol consumed in beer and mixed drinks is ethyl alcohol, a central nervous system depressant. From a medical point of view, it acts on the body much like a general anesthetic. The “dose” is generally much lower and more slowly consumed in the case of alcohol, but the basic effects on the human body are similar. Alcohol is easily and quickly absorbed by the digestive tract. The bloodstream absorbs about 80 to 90 percent of the alcohol in a drink within 30 minutes when ingested on an empty stomach. The body requires about 3 hours to rid itself of all the alcohol contained in one mixed drink or one beer.
While experiencing a hangover, a pilot is still under the influence of alcohol. Although a pilot may think he or she is functioning normally, motor and mental response impairment is still present. Considerable amounts of alcohol can remain in the body for over 16 hours, so pilots should be cautious about flying too soon after drinking.
Altitude multiplies the effects of alcohol on the brain. When combined with altitude, the alcohol from two drinks may have the same effect as three or four drinks. Alcohol interferes with the brain’s ability to utilize oxygen, producing a form of histotoxic hypoxia. The effects are rapid because alcohol passes quickly into the bloodstream. In addition, the brain is a highly vascular organ that is immediately sensitive to changes in the blood’s composition. For a pilot, the lower oxygen availability at altitude and the lower capability of the brain to use the oxygen that is available can add up to a deadly combination.
Intoxication is determined by the amount of alcohol in the bloodstream. This is usually measured as a percentage by weight in the blood. 14 CFR part 91 requires that blood alcohol level be less than .04 percent and that 8 hours pass between drinking alcohol and piloting an aircraft. A pilot with a blood alcohol level of .04 percent or greater after 8 hours cannot fly until the blood alcohol falls below that amount. Even though blood alcohol may be well below .04 percent, a pilot cannot fly sooner than 8 hours after drinking alcohol. Although the regulations are quite specific, it is a good idea to be more conservative than the regulations.
UA.V.E.K3 Prescription and over-the-counter medication (FAA-H-8083-25C Ch. 17)
There are several thousand medications currently approved by the U.S. Food and Drug Administration (FDA), not including OTC (over the counter) drugs. Virtually all medications have the potential for adverse side effects in some people. Additionally, herbal and dietary supplements, sport and energy boosters, and some other “natural” products are derived from substances often found in medications that could also have adverse side effects. While some individuals experience no side effects with a particular drug or product, others may be noticeably affected. The FAA regularly reviews FDA and other data to assure that medications found acceptable for aviation duties do not pose an adverse safety risk. Drugs that cause no apparent side effects on the ground can create serious problems at even relatively low altitudes. Even at typical general aviation altitudes, the changes in concentrations of atmospheric gases in the blood can enhance the effects of seemingly innocuous drugs that can result in impaired judgment, decision-making, and performance. In addition, fatigue, stress, dehydration, and inadequate nutrition can increase an airman’s susceptibility to adverse effects from various drugs, even if they appeared to tolerate them in the past. If multiple medications are being taken at the same time, the adverse effects can be even more pronounced.
Another important consideration is that the medical condition for which a medication is prescribed may itself be disqualifying. The FAA will consider the condition in the context of risk for medical incapacitation, and the medication as well for cognitive impairment, and either or both could be found unacceptable for medical certification.
Some of the most commonly used OTC drugs, antihistamines and decongestants, have the potential to cause noticeable adverse side effects, including drowsiness and cognitive deficits. The symptoms associated with common upper respiratory infections, including the common cold, often suppress a pilot’s desire to fly, and treating symptoms with a drug that causes adverse side effects only compounds the problem. Particularly, medications containing diphenhydramine (e.g., Benadryl) are known to cause drowsiness and have a prolonged half-life, meaning the drugs stay in one’s system for an extended time, which lengthens the time that side effects are present.
Many medications, such as tranquilizers, sedatives, strong pain relievers, and cough suppressants, have primary effects that may impair judgment, memory, alertness, coordination, vision, and the ability to make calculations. Others, such as antihistamines, blood pressure drugs, muscle relaxants, and agents to control diarrhea and motion sickness, have side effects that may impair the same critical functions. Any medication that depresses the nervous system, such as a sedative, tranquilizer, or antihistamine, can make a pilot more susceptible to hypoxia.
Painkillers are grouped into two broad categories: analgesics and anesthetics. Analgesics are drugs that reduce pain, while anesthetics are drugs that deaden pain or cause loss of consciousness.
Over-the-counter analgesics, such as acetylsalicylic acid (aspirin), acetaminophen (Tylenol), and ibuprofen (Advil), have few side effects when taken in the correct dosage. Although some people are allergic to certain analgesics or may suffer from stomach irritation, flying usually is not restricted when taking these drugs. However, flying is almost always precluded while using prescription analgesics, such as drugs containing propoxyphene (e.g., Darvon), oxycodone (e.g., Percodan), meperidine (e.g., Demerol), and codeine, since these drugs are known to cause side effects, such as mental confusion, dizziness, headaches, nausea, and vision problems.
UA.V.E.K4 Hyperventilation (FAA-H-8083-25C Ch. 17)
Hyperventilation is the excessive rate and depth of respiration leading to abnormal loss of carbon dioxide from the blood. This condition occurs more often among pilots than is generally recognized. It seldom incapacitates completely, but it causes disturbing symptoms that can alarm the uninformed pilot. In such cases, increased breathing rate and anxiety further aggravate the problem. Hyperventilation can lead to unconsciousness due to the respiratory system’s overriding mechanism to regain control of breathing.
Pilots encountering an unexpected stressful situation may subconsciously increase their breathing rate. If flying at higher altitudes, either with or without oxygen, a pilot may have a tendency to breathe more rapidly than normal, which often leads to hyperventilation.
Since many of the symptoms of hyperventilation are similar to those of hypoxia, it is important to correctly diagnose and treat the proper condition. If using supplemental oxygen, check the equipment and flow rate to ensure the symptoms are not hypoxia related. Common symptoms of hyperventilation include:
• Visual impairment
• Unconsciousness
• Lightheaded or dizzy sensation
• Tingling sensations
• Hot and cold sensations
• Muscle spasms
The treatment for hyperventilation involves restoring the proper carbon dioxide level in the body. Breathing normally is both the best prevention and the best cure for hyperventilation. In addition to slowing the breathing rate, breathing into a paper bag or talking aloud helps to overcome hyperventilation. Recovery is usually rapid once the breathing rate is returned to normal.
UA.V.E.K5 Stress and fatigue (FAA-H-8083-25C Ch. 17)
Stress
Stress is the body’s response to physical and psychological demands placed upon it. The body’s reaction to stress includes releasing chemical hormones (such as adrenaline) into the blood and increasing metabolism to provide more energy to the muscles. Blood sugar, heart rate, respiration, blood pressure, and perspiration all increase. The term “stressor” is used to describe an element that causes an individual to experience stress. Examples of stressors include physical stress (noise or vibration), physiological stress (fatigue), and psychological stress (difficult work or personal situations).
Stress falls into two broad categories: acute (short term) and chronic (long term). Acute stress involves an immediate threat that is perceived as danger. This is the type of stress that triggers a “fight or flight” response in an individual, whether the threat is real or imagined. Normally, a healthy person can cope with acute stress and prevent stress overload. However, ongoing acute stress can develop into chronic stress.
Chronic stress can be defined as a level of stress that presents an intolerable burden, exceeds the ability of an individual to cope, and causes individual performance to fall sharply. Unrelenting psychological pressures, such as loneliness, financial worries, and relationship or work problems can produce a cumulative level of stress that exceeds a person’s ability to cope with the situation. When stress reaches these levels, performance falls off rapidly. Pilots experiencing this level of stress are not safe and should not exercise their airman privileges. Pilots who suspect they are suffering from chronic stress should consult a physician.
Fatigue
Fatigue is frequently associated with pilot error. Some of the effects of fatigue include degradation of attention and concentration, impaired coordination, and decreased ability to communicate. These factors seriously influence the ability to make effective decisions. Physical fatigue results from sleep loss, exercise, or physical work. Factors such as stress and prolonged performance of cognitive work result in mental fatigue.
Like stress, fatigue falls into two broad categories: acute and chronic. Acute fatigue is short term and is a normal occurrence in everyday living. It is the kind of tiredness people feel after a period of strenuous effort, excitement, or lack of sleep. Rest after exertion and 8 hours of sound sleep ordinarily cures this condition.
A special type of acute fatigue is skill fatigue. This type of fatigue has two main effects on performance:
• Timing disruption—appearing to perform a task as usual, but the timing of each component is slightly off. This makes the pattern of the operation less smooth because the pilot performs each component as though it were separate, instead of part of an integrated activity.
• Disruption of the perceptual field—concentrating attention upon movements or objects in the center of vision and neglecting those in the periphery. This is accompanied by loss of accuracy and smoothness in control movements.
Acute fatigue has many causes, but the following are among the most important for the pilot:
• Mild hypoxia (oxygen deficiency)
• Physical stress
• Psychological stress
• Depletion of physical energy resulting from psychological stress
• Sustained psychological stress
Sustained psychological stress accelerates the glandular secretions that prepare the body for quick reactions during an emergency. These secretions make the circulatory and respiratory systems work harder, and the liver releases energy to provide the extra fuel needed for brain and muscle work. When this reserve energy supply is depleted, the body lapses into generalized and severe fatigue.
Acute fatigue can be prevented by proper diet and adequate rest and sleep. A well-balanced diet prevents the body from needing to consume its own tissues as an energy source. Adequate rest maintains the body’s store of vital energy.
Chronic fatigue, extending over a long period of time, usually has psychological roots, although an underlying disease is sometimes responsible. Continuous high-stress levels produce chronic fatigue. Chronic fatigue is not relieved by proper diet and adequate rest and sleep and usually requires treatment by a physician. An individual may experience this condition in the form of weakness, tiredness, palpitations of the heart, breathlessness, headaches, or irritability. Sometimes chronic fatigue even creates stomach or intestinal problems and generalized aches and pains throughout the body. When the condition becomes serious enough, it leads to emotional illness.
If suffering from acute fatigue, stay on the ground. If fatigue occurs in the flight deck, no amount of training or experience can overcome the detrimental effects. Getting adequate rest is the only way to prevent fatigue from occurring. Avoid flying without a full night’s rest, after working excessive hours, or after an especially exhausting or stressful day. Pilots who suspect they are suffering from chronic fatigue should consult a physician.
UA.V.E.K6 Factors affecting vision (FAA-H-8083-25C Ch. 17)
Self-Imposed Stress
Night flight can be more fatiguing and stressful than day flight, and many self- imposed stressors can limit night vision. Pilots can control this type of stress by knowing the factors that can cause self-imposed stressors. Some of these factors are listed in the following paragraphs.
Alcohol
Alcohol is a sedative and its use impairs both coordination and judgment. As a result, pilots who are impaired by alcohol fail to apply the proper techniques of night vision. They are likely to stare at objects and to neglect scanning techniques. The amount of alcohol consumed determines the degree to which night vision is affected. The effects of alcohol are long lasting and the residual effects of alcohol can also impair visual scanning efficiency.
Tobacco
Of all the self-imposed stressors, cigarette smoking most decreases visual sensitivity at night. Smoking significantly increases the amount of carbon monoxide carried by the hemoglobin in red blood cells. This reduces the blood’s capacity to combine with oxygen, so less oxygen is carried in the blood. Hypoxia caused by carbon monoxide poisoning affects peripheral vision and dark adaptation. The results are the same as those for hypoxia caused by high altitude. Smoking 3 cigarettes in rapid succession or 20 to 30 cigarettes within a 24-hour period may saturate from 8 to 10 percent of the capacity of hemoglobin. Smokers lose 20 percent of their night vision capability at sea level, which is equal to a physiological altitude of 5,000 feet.
Hypoglycemia and Nutritional Deficiency
Missing or postponing meals can cause low blood sugar, which impairs night flight performance. Low blood sugar levels may result in stomach contractions, distraction, breakdown in habit pattern, and a shortened attention span. Likewise, an insufficient consumption of vitamin A may also impair night vision. Foods high in vitamin A include eggs, butter, cheese, liver, apricots, peaches, carrots, squash, spinach, peas, and most types of greens. High quantities of vitamin A do not increase night vision but a lack of vitamin A certainly impairs it.
UA.V.E.K7 Fitness for flight (AC 107-2A)
5.6 Medical Condition
Being able to operate the small unmanned aircraft safely relies on, among other things, the physical and mental capabilities of the remote PIC, person manipulating the controls, VO, and any other direct participant in the small UAS operation. Though the person manipulating the controls of a small unmanned aircraft and VO are not required to obtain an airman medical certificate, they cannot participate in the operation of a small UAS if they know or have reason to know that they have a physical or mental condition that could interfere with the safe operation of the small UAS (§ 107.17).
5.6.1 Physical or Mental Incapacitations. Obvious examples of physical or mental incapacitations that could render a remote PIC, person manipulating the controls, or VO incapable of performing their small UAS operational duties include, but are not limited to, such things as:
1. The temporary or permanent loss of the dexterity necessary to operate the CS to control the small unmanned aircraft safely.
2. The inability to maintain the required “see and avoid” vigilance due to blurred vision.
3. The inability to maintain proper situational awareness of the small unmanned aircraft operations due to illness and/or medication(s), such as after taking medications that caution against driving or operating heavy machinery.
4. A debilitating physical condition, such as a migraine headache or moderate or severe body ache(s) or pain(s) that would render the remote PIC, person manipulating the controls, or VO unable to perform small UAS operational duties.
5. A hearing or speaking impairment that would inhibit the remote PIC, person manipulating the controls, or VO from effectively communicating with each other. In such a situation, the remote PIC must ensure he or she implements an alternative means of effective communication. For example, a person who is hearing impaired may be able to use sign language to communicate effectively.
5.16 Operations While Impaired.
Part 107 does not allow operation of a small UAS if the remote PIC, person manipulating the controls, or VO is unable to carry out his or her responsibilities safely (§ 107.27). It is the remote PIC’s responsibility to ensure all crewmembers are not impaired while participating in the operation. While drug and alcohol use are known to impair judgment, certain over-the-counter medications and medical conditions could also affect the ability to operate a small unmanned aircraft safely. For example, certain antihistamines and decongestants may cause drowsiness. Additionally, part 107 prohibits a person from serving as a remote PIC, VO, or other crewmember, or manipulating the controls, if he or she:
• Consumed any alcoholic beverage within the preceding 8 hours;
• Is under the influence of alcohol;
• Has a blood alcohol concentration of .04 percent or greater; or
• Is using a drug that affects the person’s mental or physical capabilities (§ 91.17).
5.16.1 Medical Conditions. Certain medical conditions, such as epilepsy, may also create a risk to operations. It is the responsibility of remote PICs to determine that their medical condition is under control and they can safely conduct a small UAS operation.
UA.V.E.K8 Physiological aspects of night operation (FAA-H-8083-25C Ch. 17)
Vision in Flight
Of all the senses, vision is the most important for safe flight. Most of the things perceived while flying are visual or heavily supplemented by vision. As remarkable and vital as it is, vision is subject to limitations, such as illusions and blind spots. The more a pilot understands about the eyes and how they function, the easier it is to use vision effectively and compensate for potential problems. The eye functions much like a camera. Its structure includes an aperture, a lens, a mechanism for focusing, and a surface for registering images. Light enters through the cornea at the front of the eyeball, travels through the lens, and falls on the retina. The retina contains light sensitive cells that convert light energy into electrical impulses that travel through nerves to the brain. The brain interprets the electrical signals to form images. There are two kinds of light-sensitive cells in the eyes: rods and cones.
The cones are responsible for all color vision, from appreciating a glorious sunset to discerning the subtle shades in a fine painting. Cones are present throughout the retina, but are concentrated toward the center of the field of vision at the back of the retina. There is a small pit called the fovea where almost all the light sensing cells are cones. This is the area where most “looking” occurs (the center of the visual field where detail, color sensitivity, and resolution are highest).
While the cones and their associated nerves are well suited to detecting fine detail and color in high light levels, the rods are better able to detect movement and provide vision in dim light. The rods are unable to discern color but are very sensitive at low-light levels. The trouble with rods is that a large amount of light overwhelms them, and they take longer to “reset” and adapt to the dark again. There are so many cones in the fovea that are at the very center of the visual field but virtually has no rods at all. So in low light, the middle of the visual field is not very sensitive, but farther from the fovea, the rods are more numerous and provide the major portion of night vision.
Night Vision
There are many good reasons to fly at night, but pilots must keep in mind that the risks of night flying are different than during the day and often times higher. Pilots who are cautious and educated on night-flying techniques can mitigate those risks and become very comfortable and proficient in the task.
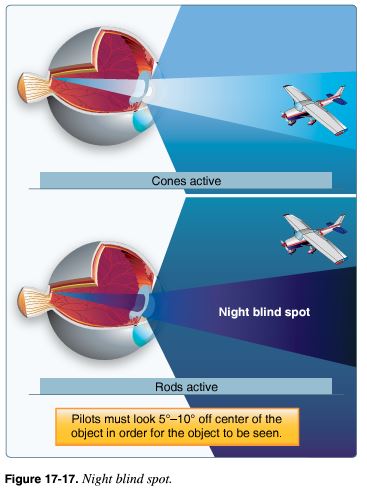
Night Blind Spot
It is estimated that once fully adapted to darkness, the rods are 10,000 times more sensitive to light than the cones, making them the primary receptors for night vision. Since the cones are concentrated near the fovea, the rods are also responsible for much of the peripheral vision. The concentration of cones in the fovea can make a night blind spot in the center of the field of vision. To see an object clearly at night, the pilot must expose the rods to the image. This can be done by looking 5° to 10° off center of the object to be seen. This can be tried in a dim light in a darkened room. When looking directly at the light, it dims or disappears altogether. When looking slightly off center, it becomes clearer and brighter.
When looking directly at an object, the image is focused mainly on the fovea, where detail is best seen. At night, the ability to see an object in the center of the visual field is reduced as the cones lose much of their sensitivity and the rods become more sensitive. Looking off center can help compensate for this night blind spot. Along with the loss of sharpness (acuity) and color at night, depth perception and judgment of size may be lost.
Dark Adaptation
Dark adaptation is the adjustment of the human eye to a dark environment. That adjustment takes longer depending on the amount of light in the environment that a person has just left. Moving from a bright room into a dark one takes longer than moving from a dim room and going into a dark one.
While the cones adapt rapidly to changes in light intensities, the rods take much longer. Walking from bright sunlight into a dark movie theater is an example of this dark adaptation period experience. The rods can take approximately 30 minutes to fully adapt to darkness. A bright light, however, can completely destroy night adaptation, leaving night vision severely compromised while the adaptation process is repeated.
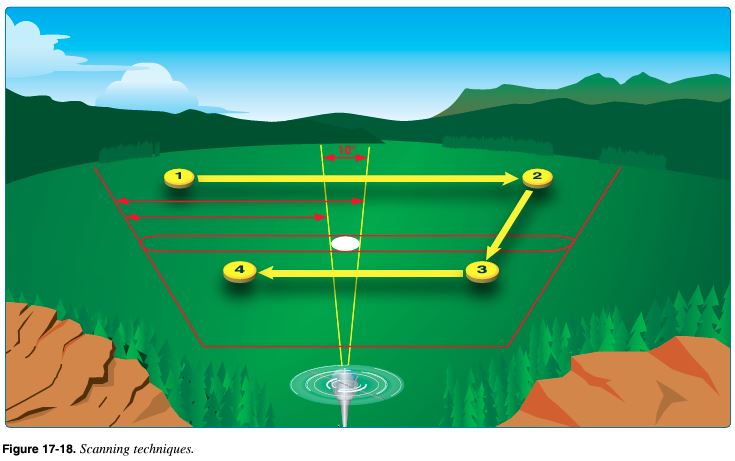
Scanning Techniques
Scanning techniques are very important in identifying objects at night. To scan effectively, pilots must look from right to left or left to right. They should begin scanning at the greatest distance an object can be perceived (top) and move inward toward the position of the aircraft (bottom). For each stop, an area approximately 30° wide should be scanned. The duration of each stop is based on the degree of detail that is required, but no stop should last longer than 2 to 3 seconds. When moving from one viewing point to the next, pilots should overlap the previous field of view by 10°.
Off-center viewing is another type of scan that pilots can use during night flying. It is a technique that requires an object be viewed by looking 10° above, below, or to either side of the object. [Figure 17-19] In this manner, the peripheral vision can maintain contact with an object.
With off-center vision, the images of an object viewed longer than 2 to 3 seconds will disappear. This occurs because the rods reach a photochemical equilibrium that prevents any further response until the scene changes. This produces a potentially unsafe operating condition. To overcome this night vision limitation, pilots must be aware of the phenomenon and avoid viewing an object for longer than 2 or 3 seconds. The peripheral field of vision will continue to pick up the object when the eyes are shifted from one off-center point to another.
UA.V.E.K9 Night illusions (FAA-H-8083-25C Ch. 17)
There are many different types of visual illusions that commonly occur at night. Anticipating and maintaining awareness of them is usually the best way to avoid them.
Autokinesis
Autokinesis is caused by staring at a single point of light against a dark background for more than a few seconds. After a few moments, the light appears to move on its own. Apparent movement of the light source will begin in about 8 to 10 seconds. To prevent this illusion, focus the eyes on objects at varying distances and avoid fixating on one source of light. This illusion can be eliminated or reduced by visual scanning, by increasing the number of lights, or by varying the light intensity. The most important of the three solutions is visual scanning. A light or lights should not be stared at for more than 10 seconds.
False Horizon
A false horizon can occur when the natural horizon is obscured or not readily apparent. It can be generated by confusing bright stars and city lights. It can also occur while flying toward the shore of an ocean or a large lake. Because of the relative darkness of the water, the lights along the shoreline can be mistaken for stars in the sky.
Reversible Perspective Illusion
At night, an aircraft may appear to be moving away from a second aircraft when it is, in fact, approaching a second aircraft. This illusion often occurs when an aircraft is flying parallel to another’s course. To determine the direction of flight, pilots should observe aircraft lights and their relative position to the horizon. If the intensity of the lights increases, the aircraft is approaching; if the lights dim, the aircraft is moving away.
Size-Distance Illusion
This illusion results from viewing a source of light that is increasing or decreasing in luminance (brightness). Pilots may interpret the light as approaching or retreating.
Fascination (Fixation)
This illusion occurs when pilots ignore orientation cues and fix their attention on a goal or an object. Student pilots tend to have this happen when they are concentrating on the aircraft instruments or attempting to land. They become fixated on one task and forget to look at what is going on around them. At night, this can be especially dangerous because aircraft ground-closure rates are difficult to determine, and there may be minimal time to correct the situation.
Flicker Vertigo
A light flickering at a rate between 4 and 20 cycles per second can produce unpleasant and dangerous reactions. Such conditions as nausea, vomiting, and vertigo may occur. On rare occasions, convulsions and unconsciousness may also occur. Proper scanning techniques at night can prevent pilots from getting flicker vertigo.
